Beyond Screening: Why Dissociation Requires Comprehensive Clinical Interviewing

Dissociation remains one of the most misunderstood and under-assessed dimensions of trauma treatment.
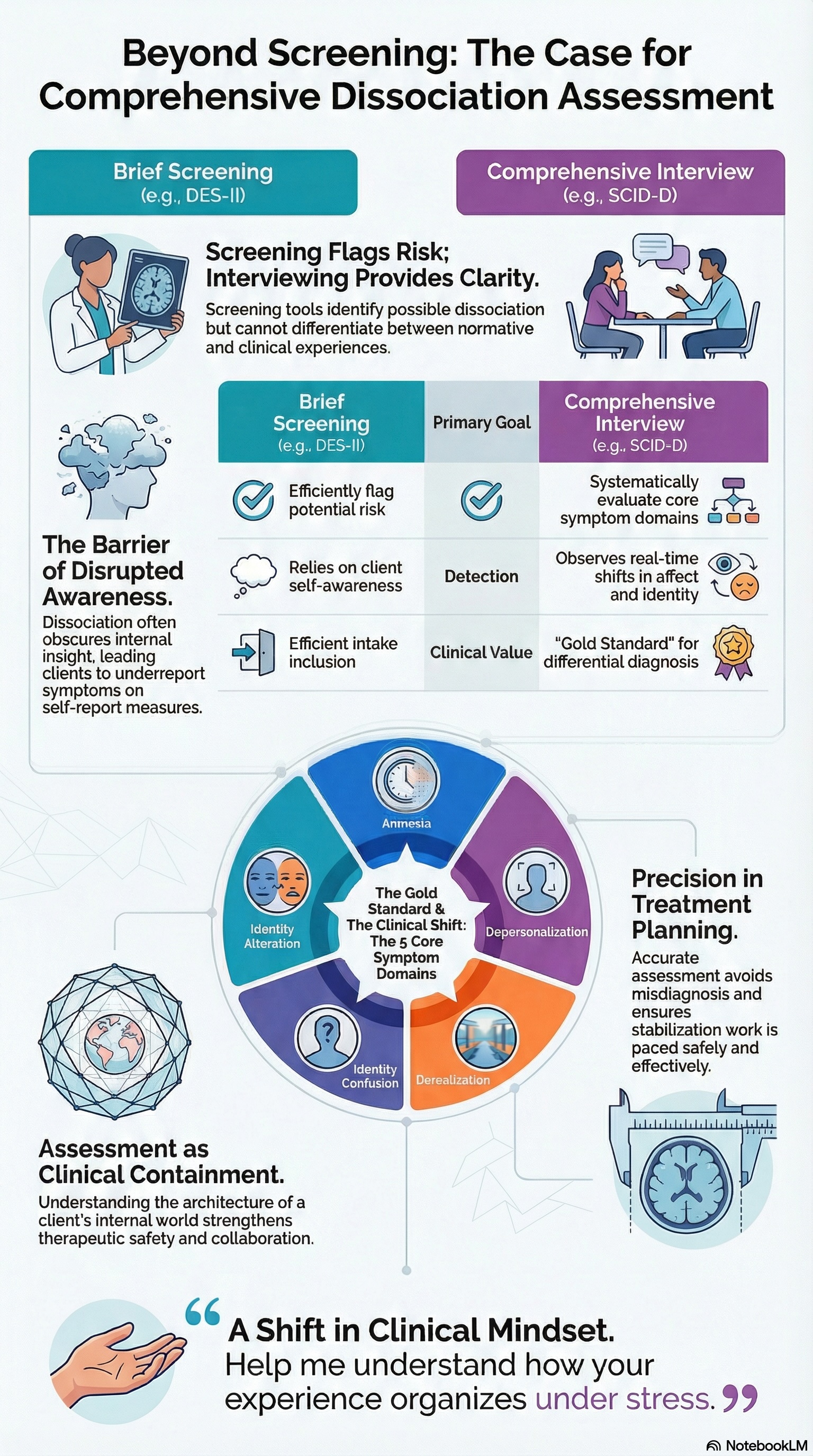
In many training programs, trauma-related dissociation and child maltreatment receive limited attention. As a result, dissociation may never meaningfully enter case conceptualization at all. In other settings, clinicians rely on assumptions about how dissociation “should” look from the outside. And in others, dissociative symptoms are screened using brief self-report measures.
Tools like the DES-II can be helpful. They are efficient, accessible, and often included in intake packets.
But here is the important distinction:
Screening is not assessment.
When dissociation is complex, chronic, or trauma-related, screening tools alone cannot help us understand its structure, severity, or clinical implications. It can be hidden, with its meaning and experience subjective to the person experiencing it.
To move from suspicion to clarity, dissociation requires comprehensive clinical interviewing.
The Limits of Screening
Screening tools are designed to flag possible risk. They are not designed to differentiate between:
- Normative dissociative experiences and clinically significant dissociation
- PTSD with dissociative features and dissociative disorders
- Depersonalization, derealization, identity alteration, amnesia, or voice hearing
- Transient stress responses and structurally organized dissociation
There is another complication.
Self-report measures depend on a client’s awareness of their own internal experience. But dissociation often involves disruptions in awareness itself.
- Clients may underreport because their experiences feel normal.
- They may not have language for what is happening internally.
- They may confuse dissociation with anxiety, inattention, or mood instability.
- They may minimize symptoms due to shame.
- They may even have amnesia for their own internal experiences.
And sometimes high scores simply reflect distress — without clarifying the nature or organization of the dissociation.
Without further exploration, we are left with ambiguity.
And ambiguity carries clinical consequences — especially when we are shaping case formulation and treatment planning.
Why Interviewing Matters
Dissociation is not simply a symptom.
It is an organization of experience — often an adaptive response developed in the context of overwhelming or chronic threat.
To understand dissociation, we need to explore:
- How often it occurs
- How intense it is
- What triggers it
- How it impacts daily functioning
- Whether amnesia or time loss is present
- Whether there is discontinuity of self-experience
- How internal voices or dialogue function
- How executive control shifts under stress
These nuances intersect and overlap. They unfold in context. They cannot be captured fully through checklists.
Comprehensive clinical interviewing allows us to slow down and ask better questions. It helps us:
- Clarify symptom phenomenology
- Differentiate dissociative conditions from other trauma-related conditions
- Reduce misdiagnosis
- Pace trauma work responsibly
- Make informed decisions about stabilization and sequencing
Assessment is not separate from intervention.
It shapes the entire arc of care.
This is not solely about diagnosis. It is about identifying how dissociation is organized so treatment can be attuned, relevant, and responsive.
When dissociation is under-assessed, Phase 1 work may stall. Trauma processing may destabilize. Protective adaptations may be misinterpreted as resistance or lack of motivation.
Dissociation as a Public Health Issue
Dissociative disorders remain underrecognized despite their prevalence and impact.
Many individuals spend years — sometimes decades — in treatment before receiving an accurate diagnosis. During that time, they may receive multiple other labels and interventions that never quite fit.
The consequences are significant:
- Increased healthcare utilization
- Chronic treatment without sustained improvement
- Elevated risk of self-harm and suicidality
- Profound relational and occupational impairment
Assessment is not only about accuracy.
It is about safety and containment.
If you would like ongoing reflections on dissociation and trauma-informed assessment, you can subscribe to our email list for additional clinical tools and resources.
What Comprehensive Interviewing Offers
Semi-structured clinical interviews such as the SCID-D are considered the gold standard for assessing dissociative conditions because they systematically evaluate the five core internal symptom domains:
- Amnesia
- Depersonalization
- Derealization
- Identity confusion
- Identity alteration
A comprehensive interview does not reduce dissociation to a score.
It allows us to observe process — shifts in affect, continuity of self, relational responses — in real time. It invites narrative detail. It clarifies subjective experience.
Importantly, interviewing is not about pathologizing.
It is about therapeutic identification. It is about understanding the architecture of a client’s internal world so that treatment can be paced and structured appropriately.
When we understand dissociation at this level, we can:
- Modify stabilization work
- Anticipate structural barriers in trauma processing
- Reduce reenactment within the therapeutic relationship
- Strengthen collaboration and safety
In this way, assessment becomes a form of clinical containment.
Moving Beyond “Do You Dissociate?”
Asking a client if they dissociate is rarely sufficient. It is also unclear what we mean when we ask that question.
Many clients will say no, while describing time loss, depersonalization, internal voices, or identity discontinuity moments later.
Comprehensive interviewing shifts the question from:
“Do you dissociate?”
to
“Help me understand how your experience organizes under stress.”
That shift matters.
It reduces shame.
It increases precision.
It creates space for complexity.
A Relational Lens on Assessment
Assessment itself is relational.
Clients with dissociative conditions often have histories of chronic relational trauma. The way we ask questions matters. The pacing of inquiry matters. Our own nervous system regulation matters.
Interviewing requires:
- Tolerance for ambiguity
- Comfort discussing identity and discontinuity
- The ability to stay grounded while exploring fragmentation
- Awareness of countertransference and therapist activation
Assessment is not merely diagnostic.
It is developmental work. It begins the therapeutic journey toward self-understanding and integration.
A Beginning, Not an Endpoint
This reflection is not suggesting that every clinician must immediately administer a full semi-structured interview.
It is an invitation to pause and ask whether screening alone is sufficient when dissociation is suspected.
When symptoms are complex, comprehensive interviewing may be necessary to move forward ethically and effectively.
And to be clear: we are not treating dissociation to eliminate it.
We are identifying the aspects of dissociation that cause distress or impairment, so that new, time-oriented strategies can be developed when circumstances have changed.
For clinicians interested in deepening their competence in dissociation assessment, the 10th Annual SCID-D Interview training will be held in summer 2026. Details will be shared in the coming months.
If you would like deeper reflections on dissociation, trauma assessment, and phase-based treatment — including clinical handouts and practice tools — you can subscribe here: Click Here
Accurate assessment is not a luxury in trauma treatment.
It is an ethical form of clinical containment and care.
Phoenix Arise Consulting
References
Boyer, S. M., Caplan, J. E., & Edwards, L. K. (2022). Trauma-related dissociation and the dissociative disorders: Neglected symptoms with severe public health consequences. Delaware journal of public health, 8(2), 78.
Leeds, A. M., Madere, J. A., & Coy, D. M. (2023). Beyond the DES-II: Screening for dissociative disorders in EMDR therapy. Journal of EMDR Practice and Research, 16(1), 25-38.
Nester, M. S., Spicher, B., Pierorazio, N. A., Brand, B. L., & McEwen, L. E. (2024). Coverage of child maltreatment in undergraduate psychopathology textbooks. Psychological trauma: theory, research, practice, and policy.
Steinberg, M. (2023). The SCID-D interview: Dissociation assessment in therapy, forensics, and research. American Psychiatric Pub.
Steinberg, M. (1995). Handbook for the Assessment of Dissociation: A Clinical Guide. American Psychiatric Press.
Steinberg, M. (1994, under development). Interviewer’s Guide to the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D). American Psychiatric Press.